Read this if you’re building HIPAA compliant software and systems and want to use AI agents
This is an update to a case study I originally shared on NoCode.tech about bringing no-code (now known as vibe-code) into a regulated healthcare org (patient portal + care-team workflows, built to move fast without letting PHI leak into the wrong tools). See the original write-up here: https://www.nocode.tech/article/i-helped-implement-no-code-with-a-healthcare-org-heres-what-i-learned
What’s different now is not HIPAA. It’s the shape of the risk when AI agents enter the system.
- The old rule still stands: only the systems that touch PHI need to be HIPAA ready.
- The new reality: agents touch more systems, faster, with less friction. Boundaries and audit trails matter more than ever.
- If a vendor will not sign a BAA, do not let that vendor touch PHI.
Context: the no-code healthcare case study this is based on
The baseline pattern is the same as the NoCode.tech article: keep PHI inside a HIPAA appropriate boundary, and still let a small care team move quickly with no code by pushing non-PHI work into simpler tools. The stack combined internal tools, automations, and patient communications. The rule was simple: if a tool cannot protect PHI, it should never see PHI.
What changed with AI agents
The temptation now is to add an agent to every workflow. In healthcare, that is only safe if you treat the agent like a new teammate.
- Clear scope: what it can do, and what it cannot do.
- Minimal access: which systems it can reach.
- Supervision: what requires human approval.
- Accountability: a clean audit trail of what it saw, decided, and did.
Modern agent use cases (updated versions of the original workflows)
The original build used no-code tools to automate patient communication and give the care team leverage. With agents, the same workflows get smarter, but they also need tighter boundaries.
1) Patient outreach agent (SMS or email) for “didn’t complete X” follow-ups
Original idea: find patients who match a condition, then text them a reminder.
Agent upgrade:
- Pulls the cohort via a query (inside the HIPAA boundary)
- Generates a message variant per patient context (but only from approved fields)
- Sends via an approved channel tool (SMS/email)
- Logs what was sent and why, without storing PHI in general logs
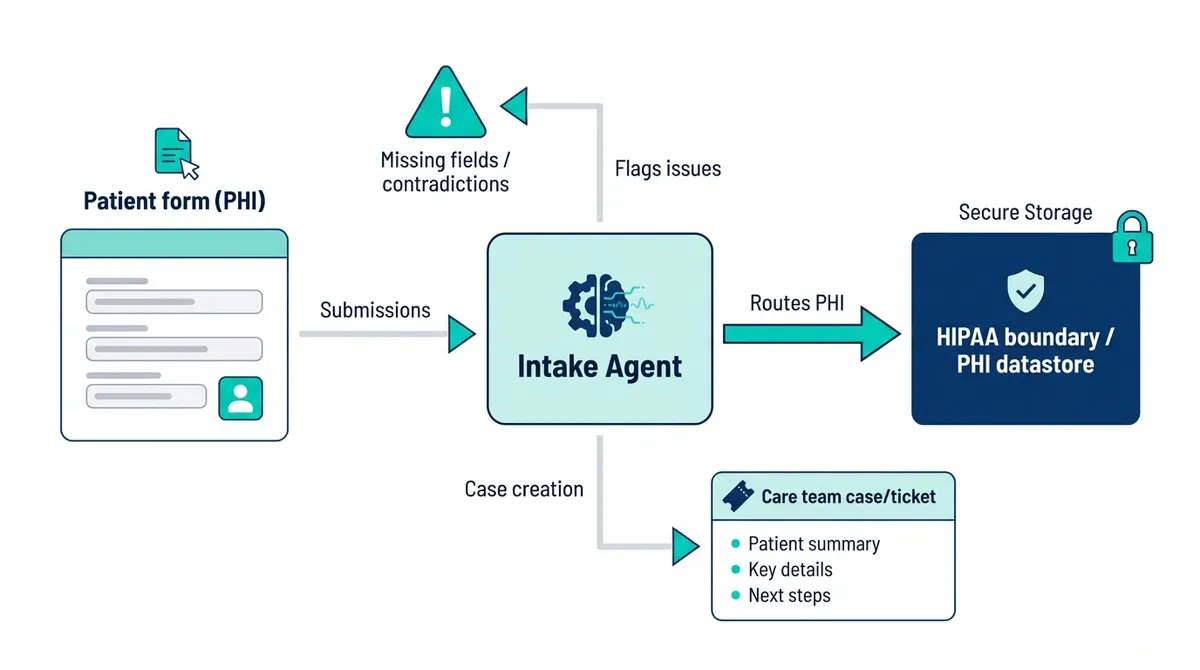
2) Intake and forms agent embedded in a marketing site
Original idea: build the website anywhere, but embed a HIPAA-capable form tool for PHI.
Agent upgrade:
- Routes form submissions (PHI) into the HIPAA boundary
- Flags missing fields or contradictory answers
- Creates a case/ticket for the care team with a structured summary
3) Care-team copilot for “one person supports hundreds of patients” operations
Original idea: a simple portal + internal tooling so a small team can handle volume.
Agent upgrade:
- Summarizes recent patient interactions into a work queue
- Suggests next-best actions (scripts, checklists, escalation paths)
- Requires approval before any outbound message or record update
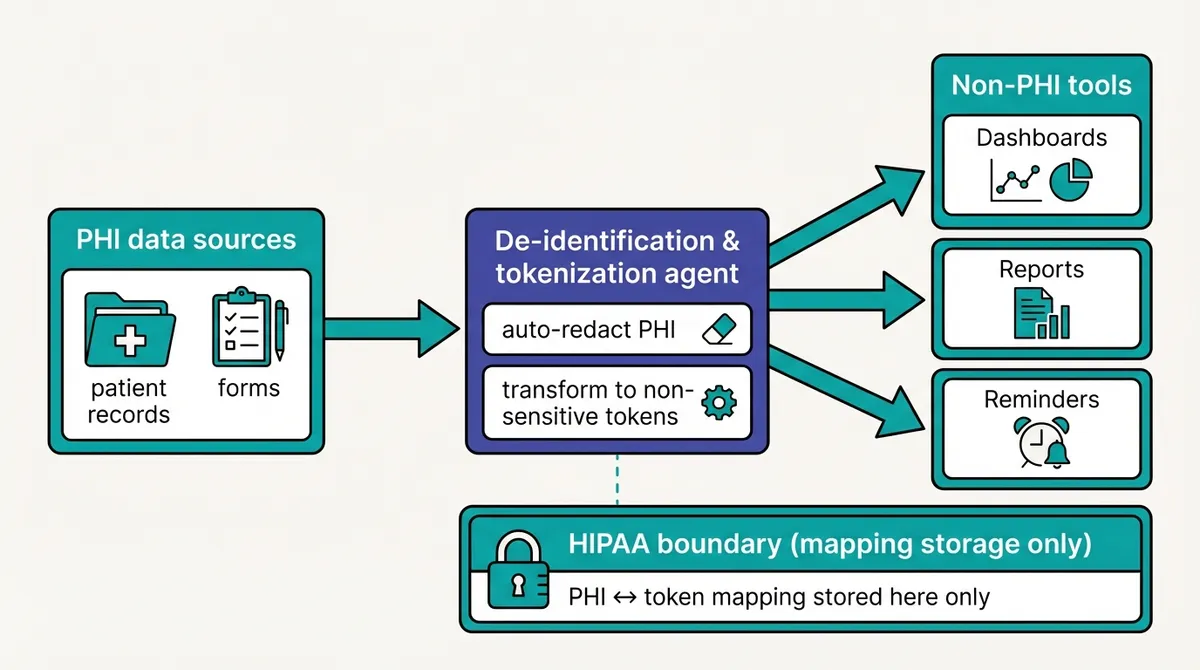
4) De-identified automation agent for non-PHI tools (the safe speed boost)
Original idea: anonymize data, then use non-HIPAA tools for convenience.
Agent upgrade:
- Auto-redacts and transforms PHI into non-sensitive tokens
- Generates operational reports, reminders, and dashboards in non-PHI systems
- Maintains a mapping only inside the HIPAA boundary
5) Documentation and training agent (keeps you audit-ready)
Original idea: document the architecture and train the team.
Agent upgrade:
- Keeps an up-to-date architecture + data-flow doc from a structured source of truth
- Generates role-based training checklists and refreshers
- Assembles audit evidence: access reviews, vendor list, policy acknowledgements
Below are the updated learnings, mapped to the original structure.
1. Audit your data flows, including agent actions
The old audit was: where does PHI exist, and where does it travel?
The updated audit is: where does PHI exist, where does it travel, and where could an agent accidentally send it?
Practical additions for 2026:
- Make a PHI data flow diagram that includes agent steps: retrieval, summarization, decisioning, tool calls, and notifications.
- Classify every field you might send to an agent: PHI, identifiers and PII, or non sensitive.
- Define PHI safe context patterns. Example: the agent works on internal IDs and de identified summaries by default, and only requests PHI inside the compliant boundary when absolutely necessary.
2. Permissions are the main battlefield
In the original article, I warned about row level permissions and not putting PHI in tools that cannot restrict access.
With agents, permissions matter even more because they can chain actions in seconds: read, decide, write, notify.
Updated best practices:
- Treat every tool an agent can call as a privileged operation.
- Use least privilege for integrations. Separate credentials per workflow, not one all access key.
- Put human approval on high impact actions: patient communications, changes to clinical records, exports, and access changes.
- Log every tool call: who requested it, what data scope was used, what the agent decided, and what external systems were touched.
3. Observability needs to be PHI safe
Everyone wants better debugging for AI. The trap is logging too much.
Updated guidance:
- Do not store raw prompts or responses containing PHI in general purpose logs.
- If you must keep transcripts for QA or compliance, store them in a controlled system with strict access, retention rules, and auditing.
- Prefer structured logs: event type, IDs, timestamps, policy decisions, and tool call metadata. Use redaction by default.
4. Document and train, now with an agent playbook
Compliance is repeatable process, as demonstrated by the rise in “compliance-as-service” companies live Vanta. HIPAA is a set of processes and checkboxes for people and machines, now including agents. The concept is not new.
What is new:
- A written agent policy that states what the agent is allowed to do, and what it must never do.
- A playbook for exceptions. What happens when the agent is unsure or the data is incomplete?
- Regular reviews: vendor terms, integration permissions, incident drills, and sampling of agent outputs.
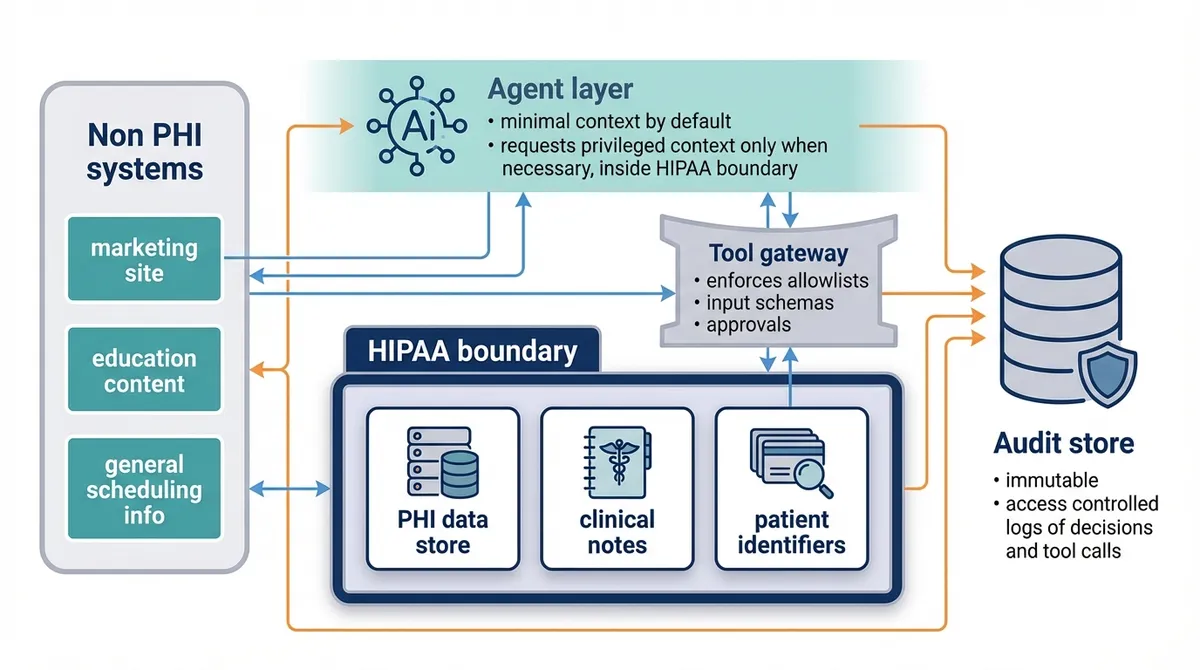
A simple reference architecture for agentic workflows
If you want a usable mental model, start here:
- Non PHI systems: marketing site, education content, general scheduling info.
- HIPAA boundary: PHI data store, clinical notes, patient identifiers.
- Agent layer: runs with minimal context by default, requests privileged context only when necessary, and only inside the HIPAA boundary.
- Tool gateway: enforces allowlists, input schemas, and approvals.
- Audit store: immutable, access controlled logs of decisions and tool calls.
FAQ: HIPAA and AI agents (quick answers)
Can I use AI agents with PHI under HIPAA?
Yes, but only if the full system is designed for HIPAA: the agent, its tool access, where data is stored, and every vendor that could receive PHI. Treat the agent like a teammate with credentials: least privilege, approvals for high impact actions, and audit trails.
Is ChatGPT HIPAA compliant?
The consumer app is not the default choice for PHI. In practice, HIPAA compliant use requires the right enterprise or API setup plus a signed BAA and a PHI safe architecture. If you cannot get a BAA for the exact services you use, do not send PHI.
What makes an AI vendor “HIPAA compliant”?
There is no magic badge. The practical checklist is: a signed BAA, clear data handling terms (retention, training, access), and controls you can enforce (encryption, access restrictions, logging, and deletion).
What is the biggest new risk when agents enter a healthcare workflow?
The biggest risk is uncontrolled blast radius: an agent that can see too much data or act in too many systems, plus accidental data egress (PHI leaking into prompts, logs, or third-party tools).
Permission sprawl is one common way this happens, but it’s not the only one. The practical goal is the same: keep PHI tightly bounded, keep tool access minimal, and make every action auditable.
What should we log for agentic workflows without leaking PHI?
Prefer structured audit logs over raw prompts: timestamps, event type, tool name, who requested the action, what record IDs were touched, approval outcomes, and redacted summaries. If you keep transcripts, store them in a controlled system with strict access and retention.
What is a safe starting architecture for an AI agent in healthcare?
Keep PHI in a HIPAA boundary, keep non PHI in simpler systems, and put a gateway in between that enforces allowlists, input schemas, and approvals. Add an immutable audit log that captures decisions and tool calls.